






This is a crosspost of the original, uncensored version of a post relating facts and developments related to past surgical human experiments by the German researchers Thorsten Walles and Heike Walles, linked to scandal surgeon Paolo Macchiarini, from the For Better Science blog. The crosspost has been prompted by legal threats having forced Leonid Schneider to remove relevant details regarding the German researcher team from another post, making it likely that such claims will be extended also to the article here crossposted. More details and background on how I view this development can be found here.
A similar crosspost has been made of the For Better Science post on Macchiarini that the Walles have already managed to bully Schneider into censoring, and is available here.
*** BEGINNING OF CROSSPOST (All of this is citation, of the original version of this post by Leonid Schneider):
This is the story of three tracheal transplants, performed by the husband and wife team Thorsten Walles and Heike Mertsching (now Walles), former collaborators of Paolo Macchiarini. My investigation quickly led to the Walles couple setting their lawyer on me, demanding almost €3000 immediately and up to €100,000 later. All because of a single short paragraph from this Macchiarini story, which mentioned their earlier activities. None of their current or former employers nor their lawyer chose to share any specific information about the 3 tracheal transplants, and the fate of these 3 patients.
Macchiarini and the Walleses started their tracheal transplant activities at the Medical University Hannover (MHH), under the regenerative medicine enthusiast Axel Haverich. Together, the team implanted in 2003 a tracheal patch into a cancer patient using a piece of pig intestine, and moved their separate ways soon afterwards. Macchiarini went in 2004 to Barcelona, where he had his famous trachea transplant breakthrough in 2008 (see my report here). The Walles couple went in the same year to Stuttgart in southern Germany. The thorax surgeon Thorsten to the Robert Bosch Hospital, Clinic Schillerhöhe, the regenerative medicine-specialising biologist Heike (back then carrying the name of her previous husband, Mertsching) became professor at the Fraunhofer Institute for Interfacial Engineering and Biotechnology (Fraunhofer IGB). There, the husband and wife team transplanted between 2007 and 2009 two more patients with tracheal replacements made from pig intestine. The clinical success and the actual performance of these transplants is unclear, it is also not helpful that authors chose to omit certain key aspects when the two cases were eventually published.
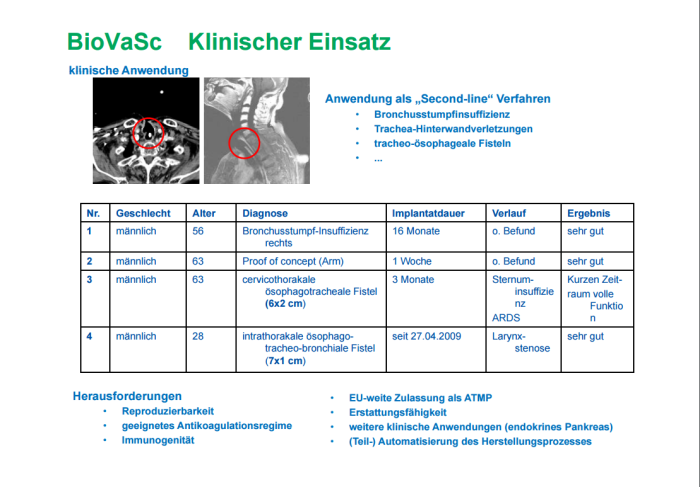
“We developed a bioartificial tissue (TraVaSc-TERM ®) for the surgical reconstruction of extensive tracheo-bronchial defects including circumferent airway replacement. The tissue is generated from a xenogene biological scaffold [pig intestine, -LS] that is decellularized, preserving the structure of the vascular network. For transplant generation, these vascular structures are reseeded with autologous endothelial precursor cells of the recipient. Two more autologous cell types are needed to generate a functional airway substitute. Our approach results in a vascularized autologous transplant tissue that can be connected to the recipient’s blood supply at time of implantation to guarantee transplant survival. Tissue generation takes about five weeks. The TraVaSc-TERM ® was applied successfully in three patients between 2006 and 2009 [actually, it seems one patient was counted as two, -LS]. As a result of the ATMP-legislation in Europe the TraVaSc-TERM ®-generation process had to be transferred from an F&E environment into GMP. This task was finished in 2015 and we wait for regulatory approval”.After her 3 allegedly successful tracheal transplants, Heike Walles became a member of the German Ethics Council (Ethikrat) In June 2010 and served the nation by safeguarding patient protection and medical ethics in Germany until September 2012. Mightily impressed by her research achievements, the federal state of Bavaria dumped in 2014 €10 Million over Heike Walles and invited her to head the new translational centre for “Regenerative Therapies for Oncology and Musculoskeletal Diseases” in Würzburg. The new director remained affiliated with her Fraunhofer institute, but additionally became in August 2009 professor at the University Clinic Würzburg. Her husband Thorsten received a professorship at the same place in January 2012. There, the couple began to collaborate with the technology giant Siemens and are apparently almost ready to churn out tissues and organs to save hundreds of patients, based on their previous success stories. As Walles’ co-worker Jan Hansmann from Fraunhofer declared in Siemens-magazine article from September 2016:
“Hansmann describes one of the major successes of tissue engineering in Würzburg: “Working with the University Hospital and the Robert Bosch Hospital, we recently produced a complete section of a human windpipe in the bioreactor and successfully implanted it into a very seriously ill patient as part of a ‘compassionate use’ program.” In fact, no other research group in the world has to date produced such a complex biological implant”.
Silent night
The case of that and other two tracheal transplants was very tangled. At points, my perception was that the publicly owned German research institutions deliberately wanted me to follow false leads I picked up on internet, in order to discredit my reporting. Indeed, the fact that the Walleses used their official University Clinic Würzburg affiliations in the lawyer’s letter suggests an involvement of their employer, who received (but never really answered) my questions 2 weeks before my previous article appeared. That would be indeed an interesting new way for a German university to react to a blogger’s inquiry.The current Walles employers, University of Würzburg and the Fraunhofer Institute for Interfacial Engineering and Biotechnology (Fraunhofer IGB) chose not to share any useful information with me. Würzburg categorically denied their University Clinic’s involvement in the operation described by Hansmann above, Siemens magazine refused to explain and Hansmann never replied to my email. Thorsten Walles’ former boss, head of thorax surgery at Schillerhöhe Clinic in Stuttgart, Godehard Friedel, who co-developed the technology, forwarded my email to his PR spokesperson, who refused to share any information citing protection of patient privacy. Thus, no thanks at all go to them. In the end however, I think I could reconstruct the three trachea transplants made by the Walles couple quite truthfully.
It got that bad that the press relations offices of the Fraunhofer IGB, whose job it is to promote the institute’s research and publications, repeatedly refused to name me the papers where Walles’ three trachea transplant patients had been described. I found those anyway, and I also found out that some very important aspects have been omitted from the publications. Small issues like the suspected failure of the transplants, or these patients being long dead at the time when the papers were published.
The same Fraunhofer PR officer Claudia Vorbeck who denied me any information whatsoever, also by insisting that the federally-sponsored public research institution is exempt from Freedom of Information inquiries, authored in 2009 a press release hailing one of these Walles trachea transplants (see 3rd patient below). All I was made understand was that the Fraunhofer Institute takes enormous pride in the research of their professor Heike Walles:
“Prof. Walles develops and uses methods of tissue engineering to produce the most diverse, complex human tissues that are used for risk assessment in chemical and pharmaceutical research as well as in regenerative medicine. Prof. Walles and her team use biological carrier materials for the production of these human tissues. In the course of her research at the Fraunhofer IGB, Prof. Walles has developed a biological matrix consisting of a decellularized pig intestine as a scaffolding structure for a potential trachea implant”.Vorbeck then added:
“The research work of Prof. Walles for the development and production of trachea grafts on a biological matrix was carried out at the Fraunhofer Institute IGB according to the requirements of the German medicinal product (https://www.gesetze-im-internet.de/amg_1976/). The authorities responsible in this context were always involved in accordance with legal requirements. These authorities also have all the necessary documents on good scientific practice, such as ethics or animal welfare applications”.The University of Würzburg refuse to comment on anything which happened before Walleses became their professors. At least I managed to get this out, after some yanking:
“The professors Walles declare that the cooperation with Mr. P. Macchiarini ended already in early 2005. The last common publications stems from the year 2006“.
The first patient, or Macchiarini-led kick-off in Hannover
I reported previously about this Macchiarini operation in my article about his patients. As the local newspaper, Hannoversche Allgemeine Zeitung (HAZ) reported on September 6th 2003, Macchiarini and the Walles couple transplanted the cancer patient Ernst Fromhage with a tracheal patch of decellurised pig intestine seeded with patient’s own muscle cells. The intervention was published as MacChiarini (sic!) et al 2004 and the method as Walles et al, 2004. Macchiarini is corresponding author on both publications and thus the principal investigator chiefly responsible for the development of that technology. However, Thorsten Walles claimed the credit in a 2009 interview for himself and his wife:„In 2003, I specialized in thoracic surgery for my surgical training. Here, I first met patients with tracheal injuries that could not be treated anymore. I was able to convince my then-boss Paolo Macchiarini of the concept of treating such injuries with bioartificial tissues. Together we modified the procedures for the production of human bioartificial tissues for trachea transplants, originally developed by Prof. Mertsching and myself. Already in 2004 we were able to successfully treat the first patient”.Not everyone was impressed. The famous late thorax surgery specialist Hermes Grillo took an issue with this method (Grillo, 2005):
“One must also question placement of a free graft of any tissue over an area that is still contaminated, even if not grossly infected, by the bacteria that necessarily are present in such a situation, despite all cleanup treatment before repair. More to the point, however, is the fact that defects of this sort have long been closed by vascularized pedicled autogenous tissues (omentum, pericardium, intercostal muscle, and other muscle flaps). Addition of an engineered tissue graft seems superfluous”.Yet according to Walles, the 2003 operation on the patient Fromhage in Hannover was a success for regenerative medicine:
“The implant healed easily into the airway and there were no problems. The patient lived for 16 months a self-determined life. Unfortunately, his cancer caught up with him and he died”.Now it makes sense why back in spring 2016 the Hannover hospital refused to share with me any information about the fate of that patient, claiming that his medical records were not available.
The second patient and his half-story
Of the second patient, a 63-year old man, we do not know the name, and we do not know exactly what kind of transplant he received. This is what the 2013 book by the German journalist Bernhard Albrecht, “Patient of My Life” in its chapter “Breathing” (see Google-Books version), tells us about Walles’ tracheal transplants:“Twice they operated patients whose windpipes were corroded by cancer. Both did not live long after the operation. The first patient [Fromhage, operated together with Macchiarini in 2003, -LS] died on his main disease, but the second one began to question all their efforts. The artificial trachea rotted namely inside his body. The fault lied with the absence of own blood supply in the artificial tissue”.As Walles lawyer made clear, the artificial material was not plastic, where “the blood supply does not function”, but based on a biological scaffold. But the lawyer did not specify how the capillary blood supply inside dead decellurised scaffold is supposed to succeed. Macchiarini and his partners in Spain, Italy and UK transplanted many patients with such, using decellurised donor tracheas. It seems all these transplants either rotted and collapsed or were overgrown with scar tissue, unless you trust those authors’ own claims of vascularisation and full regeneration. It would be nice to know more about Walles’ pig intestine transplant and how it fared inside that 63-year old man’s throat, but alas, this is none of public’s business apparently. There was however this very informative interview from 2009 with Thorsten Walles with the German magazine The Stem Cell (Die Stammzelle):
“Dr. Walles: The technology was ready for operation from 2007 onwards. In the same year a patient with a combined injury from the trachea and esophagus was arrived to us from another clinic. The 63-year-old has been unable to eat, drink or speak for three years. He therefore had a tracheostomy and took his food through a stomach probe, which was introduced through his nose. In the 3 years, a total of 14 surgeries were performed by the various clinics on the patient in order to close the defect. Unfortunately, all unsuccessful. A surgeon who treated this patient had heard of our new procedure and referred the patient to us.The paper appeared as Mertsching et al 2009, but it never mentions that the one-week in-arm experiment was followed up by the actual trachea transplant into the throat. Surely that bit would have been most interesting for the worldwide community of thorax surgeons and stem cell researchers? According to Heike Walles presentation to the German Ethics Council, the transplant was “fully functional over a short period of time”.
The stem cell: And you implanted a piece of the air tube?
Dr. Walles: Not immediatedly. Due to the large defect, it was necessary to use an implant with its own vascular supply. We had never done this before in a human being and we were honestly afraid to use these new implants in the chest and risk that they would fail and cause serious complications.
The stem cell: So what did they do then?
Dr. Walles: We grew a bioartificial tissue as we needed it for the repair of the airway defect and implanted it into the left upper arm of the patient.
The stem cell: Why exactly there?
Dr. Walles: The blood vessels in the upper arm are easy to reach and do not require any major surgery. We have connected the graft to the upper arm vessels with two microsurgical vascular anastomoses. After one week we removed the transplant again and it was examined by the researchers in the Fraunhofer IGB.
The stem cell: Why?
Dr. Walles: We wanted to make sure that the artificially produced vessels work in the implant and that the transplant does not die. We have therefore clinically checked whether our implant has the function we expect at all. We also wanted to ascertain whether there were any side effects, such as, for example, inflammatory reactions occurring after rejection. We had prepared a second implant for the reconstruction of the airway and esophageal end defect, which would be ready for use 1 week after explantation of the arm implant. So we had 1 week to prove how well our technology works in humans. For this the researchers at the Fraunhofer IGB had to do night shifts. The studies showed that the transplant was fully functional even after one week. The results have now been published in the scientific journal Transplantation”.
When the Mertsching et al 2009 paper was published and when Thorsten Walles gave that interview to “The Stem Cell”, the patient had been dead for almost 2 years already. This was indirectly suggested by Heike Walles’ Ethics Council presentation, confirmed by the 2013 dissertation of her PhD student Iris Dally (page 126), as well as by a press release of the state of Baden-Württemberg from October 2008 which quoted Thorsten Walles:
“Walles does not want to rush: “We want to approach the clinical application of this method slowly.” Despite all the initial successes, transplantations are still an experimental and risky intervention. There will always be setbacks. The last patient implanted with a piece of bioartificial tissue died a few weeks after surgery as a result of unexpected complications”.Whatever their reasons to be modest, the ground-breaking tracheal replacement operation and the ensuing unexpected demise of the patient were omitted in the Mertsching et al 2009 article. What lead to his death? In his available interviews, Thorsten Walles never mentioned anything about cancer (but the Albrecht book did, see above), only a physical injury to the trachea and oesophagus, and everyone involved refused to divulge any information. It is not clear therefore why the patient died so soon after a piece of pig intestine was inserted into his chest as his new breathing tube.
The 3rd patient and another puzzle around the transplant
The interview in The Stem Cell is from August 2009, yet Walles does not mention his 3rd patient, the Indian Pavninder Singh, whom he and his wife transplanted just half a year before with a “regenerated” piece of pig intestine. Not a single word. Instead, Walles speaks of new European regulations and changes in German medicinal product regulations, which stopped his big plans:“In July 2009, we received funding from the German Federal Ministry of Education and Research (BMBF) (FKZ 0315575) to fund a clinical trial for the treatment of patients with tracheal and esophageal defects with our bioartificial transplants. First, we must provide the regulatory authorities with the information they need in order to get a manufacturer’s license at the end. Our aim is to obtain a European approval for our bioartificial tissue implants within the framework of the study”.The trial obviously never happened, lacking approval from authorities. The Walles methodology suffered a major setback when the new German medicinal produce legislation (Arzneimittelgesetz) became officially binding on July 17th 2009, less than three months after Walleses performed the third (and apparently last) trachea transplant. According to Albrecht book, the investigations by the authorities into suspected breach of regulations were therefore aborted.
Singh originally came to Germany illegally, but integrated quickly, married a German wife and learned German language. On December 9th 2008, the young man in his twenties attempted suicide by swallowing oven cleaner fluid. Singh survived, but his oesophagus and trachea were damaged irreparably. He had to be saved by tracheostomy, a permanent hole in his throat. Because of his burned epiglottis, the patient had to keep an erect posture at all times to avoid stomach acid flowing into his airways and lungs. In April 27th 2009, Singh received a tracheal transplant from the Walles couple, fashioned from pig intestine. This is how the University of Würzburg described the breakthrough achievements of their new professors:
“Thorsten Walles and his colleagues carried out the successful transplantation of the replacement trachea at the Schillerhöhe Lung Clinic in Gerlingen near Stuttgart in April 2009. The artificial organ was accepted by the body without rejection and adequately supplied with blood. Unfortunately, after this encouraging world premiere, the further development and dissemination of the procedure has been stalled due to European changes in the drug legislation”.Now however, the PR person of the University of Würzburg, Esther Knemeyer Pereira replied to my inquiry that all three tracheal transplant operations by Walles took place before 2009, and had nothing to do with the university or its clinic. At the same time, the Würzburg professors Walles operated until 2014 a personal website “Bioartificial organs”, where patients were invited to contact Thorsten Walles at Clinic Schillerhöhe about “bioartificial implants for reconstructive thoracic surgery” (screenshots of the website here). This might explain why my inquiry if further tracheal transplants are intended in Würzburg went unanswered. Meanwhile, a legal action against me was being prepared.
What Walles or their academic employers never ever mentioned: Singh’s trachea transplant most likely did not work. Shortly after the operation, Walles re-opened the tracheostomy, the hole in the throat remained until Singh’s suicide death in December 2011. This information is only available in the Albrecht book (“the hole in his throat was his misery”), because the author met the patient personally in November 2011, shortly before Singh’s accomplished suicide:
“Why does he need the hole [tracheostomy, -LS] still? Dr. Walles initially closed it, told Singh. But then he had always been chocking, food and saliva entered the windpipe. The oven cleaner had also corroded the epiglottis in his throat. Due to heavy scarring, it did not close properly when swallowing.”We do not know for sure if the transplant integrated as announced, but given the tracheostomy, it was unlikely to be of any use even if it did. Heike Walles declared to the Ethics Council in 2010 that the patient Singh “has no problems whatsoever”. Also her lawyer now sternly told me:
“The patient described in the book by Mr Albrecht lived self-determined life over a long period of time after the operation”.No mention of tracheostomy, again, but the lawyer did declare that all information in the Albrecht book was correct. Thorsten Walles himself spoke in a 2014 interview (which was recently removed from the BioRegio-Stern website, backup copy here):
“We have used a method for the treatment which we have been researching on since 2000 and where we already had initial successes in the application. Since the patient wanted the treatment and we also had the impression that he can make it, we grew a trachea from the cells of his body and implanted it successfully. Unfortunately, however, this has not improved his private situation and a few years later he then took his own life”.Asked about Singh’s suicide despite the miracle cure which allegedly restored his health, Walles elaborated:
“In the first moment, this pulled the ground from under our feet. We asked ourselves why we carried out this elaborate treatment in the first place. This experience prevented us so far from publishing our scientific results of the applied technology, because we were questioning the rationale of the treatment in this case”.The next year however, a paper was published which described a patient case perfectly fitting that of Singh. With one exception: the patient in Steinke et al, Tissue Engineering Part A, 2015, is seemingly alive and well. Where Singh killed himself 2.5 years after the operation, his published doppelgänger was examined just after the same period and was found that he “could eat and drink normally and was also able to play soccer”. No tracheostomy was mentioned, instead:
“The early postoperative course was uneventful and the transplanted airway tissue was integrated into the host. 2.5 years after transplantation, a bronchoscopy confirmed the scar-free reconstruction of the former airway defect. Histological work-up documented respiratory airway mucosa lining the bronchial reconstruction, making it indistinguishable from native airway mucosa. After transplantation, our bioartificial airway tissue provided perfect airway healing.”Was it indeed a biopsy as the authors report, or possibly an autopsy of a suicide victim? I tried to find out from the paper’s authors if the patient was indeed Singh. Walles’ PhD student Dally (who herself declared Singh as dead in her dissertation), threw down the phone on me, the corresponding author Maria Steinke, Chair of Tissue Engineering and Regenerative Medicine in Würzburg, did the same after telling me she is not entitled to comment. The Fraunhofer PR person Vorbeck declared to me that the responsibility for the content and correctness of the two discussed Walles publications featuring Fraunhofer affiliation lied predominantly with the clinicians who treated these patients. But not with Fraunhofer or their own scientist Heike Walles, who according to Vorbeck never performed any “human experimenting”.
In that Steinke et al, 2015 publication, the authors state that they did not replace a segment of trachea, but introduced a large pig-intestine-made patch of “membranous part of the trachea”. This is strange, all other sources (like this Spiegel magazine article from 2011, or even Fraunhofer own press release) clearly suggest a replacement of the tracheal tube, not a patch. What did the second patient receive then, the one who died so soon after the operation? The corresponding Mertsching et al 2009 paper clearly showed a tubular piece of pig intestine. Yet all information is kept secret by the Fraunhofer Institute, the Clinic Schillerhöhe and the University of Würzburg. Also the Walles lawyer does not speak of that unlucky 63-year old man at all.
Clinical trial cancelled?
A scheduled clinical trial with 5 patients, funded since July 2009 by the German Federal Ministry for Education and Research, and to be carried out at Clinic Schillerhöhe (see 2013 Dally dissertation, page 139) was apparently not approved and never performed (Heike Walles spoke of 15 patients in her Ethics Council presentation in 2010). A tragedy, certainly for the Fraunhofer Institute and their clinic partners, maybe less so for the patients.After the hype, these alleged successes became almost forgotten. In 2010, Thorsten Walles received a Von-Langenbeck-Award of the German Surgery Society (DGCH). The press release mentions only the first patient from Hannover, the merits are shared with Heike Walles. Paolo Macchiarini, the corresponding author of that publication, is someone whom the Walleses seem to be most reluctant to be associated with, as also the lawyer’s letter made clear.
*** END OF CROSSPOST
No comments:
Post a Comment